How We Think about Ovulation Induction at Our Clinic
How We Think about Ovulation Induction at Our Clinic
Here at Oak Clinic, we offer two courses for proceeding with ovulation induction.
“Natural”/“Body-friendly” IVF and “Active” IVF. From our many years treating patients, our approach is one of tailoring the treatment to each individual patient.
Therefore, before the oocyte pick-up cycle begins, we will devise a plan that suits each patient, based on one of these styles or the other.
Both courses offer painless IVF procedures.
Even for patients who can grow multiple oocytes, not all oocytes can be fertilized.
For example, some oocytes may be immature or have other obstacles.
Additionally, some patients do not respond well to stimulation and many follicles may not grow despite daily injections.
In cases like this, it is less burdensome to collect oocytes with a relaxed, natural cycle.
In order to do so, equipment and expertise like what we have at Oak Clinic is required to quickly perform hormone tests and collect the oocyte(s) upon release.
If this is not done smoothly and the oocyte is missed, it may be necessary to wait another month.
"Active" IVF
In "Active" IVF, the ovaries are actively stimulated by injected medication, in order to produce as many oocytes as safely possible.
This is a popular method, because many oocytes can be collected at one time, rendering overall treatment more efficient.
This is especially useful for those who are older, who have a decrease in ovarian reserve, and those who wish to adjust their oocyte pick-up date (by 1-2 days) due to their busy lifestyle.
Further reasons for popularity are as follows:
In the case of the low-stimulation or natural method, there are cases where embryo transfer is not possible due to factors like cancellation of oocyte pick-up (from spontaneous ovulation), the presence of vacuoles, or failure to fertilize. With more oocytes and control over timing, there is more opportunity for success.
In the case of the low-stimulation or natural method, the number of oocytes collected is very small, so more cycles may be required to get the desired number of oocytes. Having fewer cycles that collect more oocytes may be less burdensome to the body and also less expensive to the patient.
Many patients, especially in their late 30’s or after, wish to have more than one child, and surplus embryos can be frozen for future embryo transfers.
Recently, the HMG-MPA method (which uses oral medication for ovulation suppression) and the "short" method are very popular.
One of the advantages is that you can start at any point in your menstrual cycle, using our "random start" style.
For this reason, it is particularly enjoyed by patients who want to freeze their oocytes urgently, such as before cancer treatment.
The HMG-MPA method is also good for reducing the risk of OHSS.
We are prepared to relieve the pain during oocyte pick-up as much as possible.
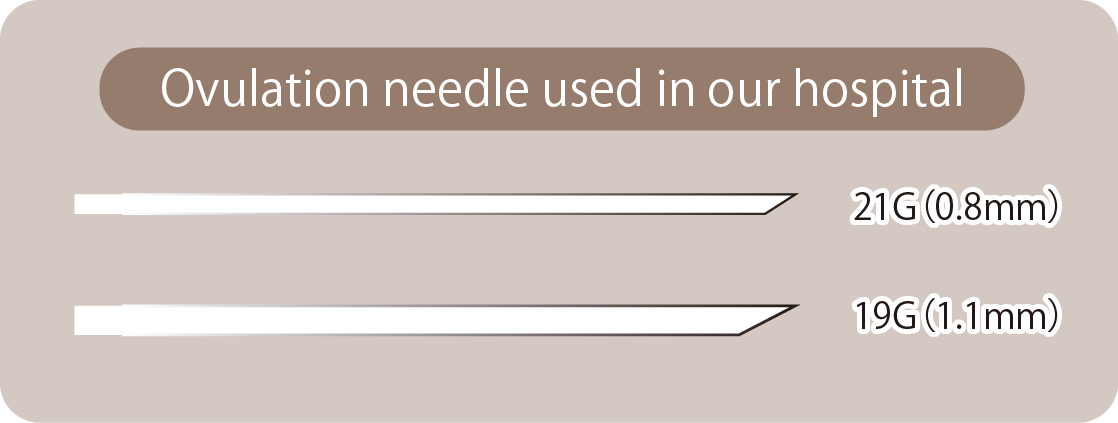
①Oocyte pick-up needle
At our hospital, the thickness of the oocyte pick-up needle is adjusted according to the number of follicles.
Some people believe that the thinner the needle, the less pain there is, but the pain of needle insertion is very brief.
On the other hand, a thinner needle takes a longer time to collect the oocytes, which may also cause discomfort.
Therefore, balance is necessary.
Generally speaking, the needle used maybe 21 gauge to 19 gauge.
② Anesthesia
In the case of a natural cycle, some facilities may collect oocytes without anesthesia due to the small number of developing follicles.
However, there is no getting around the fact that oocyte pick-up without anesthesia is a painful process, no matter the number of follicles.
The ovaries are located in the abdomen, so the needle must pass through the vaginal wall to reach and pierce the ovaries.
The vaginal wall in particular is very sensitive to pain, so local anesthesia is used to eliminate this pain in a similar way as a dentist might use anesthesia on a patient’s gums.
As the ovary itself is an organ and is impacted by systemic medication, pain associated with the ovary can be greatly relieved by inserting a suppository in advance.
It also works well when there is pain after the oocyte pick-up, not only during.
In addition, short-acting intravenous anesthesia is used to reduce or eliminate the tension from pain during oocyte pick-up, which would otherwise increase discomfort.
It also prevents the patient moving the body too much, which would make it harder to collect oocytes.
The time required for oocyte pick-up is about five minutes, so only a small amount of intravenous anesthesia is necessary. Most patients sleep through the procedure.
③ Reassuring environment
There are individual differences from person to person on how pain is experienced, but whether you have peace of mind has a great effect on the pain you feel.
We strive to reduce patient anxiety as much as possible, and you can always ask us any questions you may have.
In addition, on the day of the event, the nurse, doctor, and embryologist will each introduce themselves and confirm their identity before oocytes are collected.
Experienced Doctors & Teamwork
Our hospital is a designated training facility for reproductive medicine specialists, and a large number of specialists undergo training work with us.
Every doctor who joins us is well-trained as an obstetrician and gynecologist, and the doctors in our Osaka and Tokyo locations communicate with one another and with our senior directors.
If there is ever any uncertainty, we will also consult with the patient’s preference.
The medical record information is shared among physicians, and it is possible to exchange opinions while viewing video data of ultrasound exams on the spot.
In the clinical setting, some situations cannot easily be decided by one person.
At that time, in our hospital, the judgment is not made by a single doctor, but by our team as a whole.
Hormone Measurement Equipment
Fifteen minutes after blood collection, the following hormone results can be obtained and used immediately as an index for medical treatment.
The equipment is AIA-360 from TOSOH.
Estrogen level:Secreted from follicles, this is an indicator of follicle development.
LH:Using this hormone we can check if preovulatory follicle maturation has begun.
FSH:This helps predict ovarian response for the same cycle.
Discussion of Ovulation Induction Methods
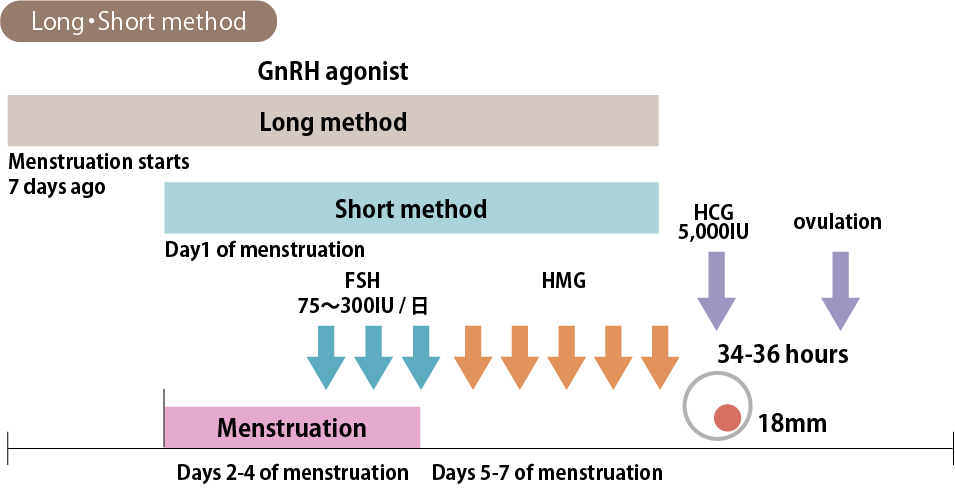
Short Method / Long Method
-Is the long method better than other methods, such as short method?-
The long agonist method of ovulation induction has become the world standard.
There has been a long debate about whether the long method or the short method is better, but as for the success rate, randomized controlled studies have indicated that the long method has some advantage overall, but only very slightly.
However, this is not always our first choice.
Reasons for this:
The long method requires the use of contraception in the previous cycle.
The use of agonists from the middle stage of the high temperature period means that there is no avoiding the use of these contraceptives.
Patients presenting with infertility often find it frustrating or unnatural to use these medications, as it deprives them of the opportunity to get pregnant in the previous cycle that they might otherwise have.
In addition, if contraception is unsuccessful and a pregnancy does occur, unnecessary drugs will have been introduced in these early stages of pregnancy.
Compared to the short method, the long method has no flare-up effect and has stronger pituitary suppression, which means it requires a larger HMG injection.
It is said that the long method permits easier adjustment of the oocyte pick-up date and reduced risk of OHSS due to stronger pituitary suppression, but only slightly.
Even with the short method, in the case of the first oocyte pick-up, this same control can be achieved with close monitoring of the follicles and adjustment of medications.
None of this is to say that the short method is definitely better or that the long method is not good, but that different methods may better suit different patients under different conditions and situations.
Most people who undergo IVF are in their late 30’s to early 40’s, when ovarian reserve and the proportion of good oocytes is reduced and people’s lives are busy.
Many patients hope to adjust their own oocyte pick-up date (by 1-2 days) and to secure many frozen oocytes.
The best method can be decided for each individual patient.
Agonist/Antagonist(Cetrotide®)or MPA
Historically, the conventional method was to suppress ovulation with an agonist (mainly nasal drops for the short method/long method) and collect oocytes, but antagonists that can temporarily suppress ovulation have since entered use, around ten years ago.
Until the current formulation was developed, however, strong side effects rendered it unpopular.
(New formulations are gentler.)
In the stimulation cycle, use starts on the sixth day.
At the beginning of formulation, it was reported that the quality of oocytes collected by antagonist use was better than that of agonists, but developments since then have rendered the quality of oocytes the same by either method.
It is the same at our hospital.
With antagonists, there is weak pituitary suppression and the effect is more temporary.
On the other hand, there is more risk of spontaneous ovulation.
So, for example, when there are several follicles with different sizes (some of which are growing slowly) the agonist method firmly suppresses ovulation until all follicles are sufficient size.
Then you can wait for the development of small follicles.
However, with the antagonist method, it becomes difficult for large follicles to ovulate, so you cannot wait for too long.
As a result, there are cases where the agonist method may be able to recover more oocytes.